News
Cancer Clinical Trials – how they have evolved and what we can expect in the future
In 2023, World Cancer Day looks at highlighting the progress that has been made so far with cancer treatment. In this article, Compass Life Sciences looks at diversity representation within cancer clinical trials and how these have advanced over the last decade.
Clinical trial results from the last decade
Few cancer trials included enough non-white or older patients to be truly representative, according to a new scorecard published in BMJ Medicine showing how well pharma companies diversify research studies. The non-profit Bioethics International analysed 64 pivotal trials conducted by 25 pharma companies of novel cancer therapeutics approved by the FDA between 2012-2017 to see how inclusive those studies were, and how transparent companies were in reporting participant demographics.
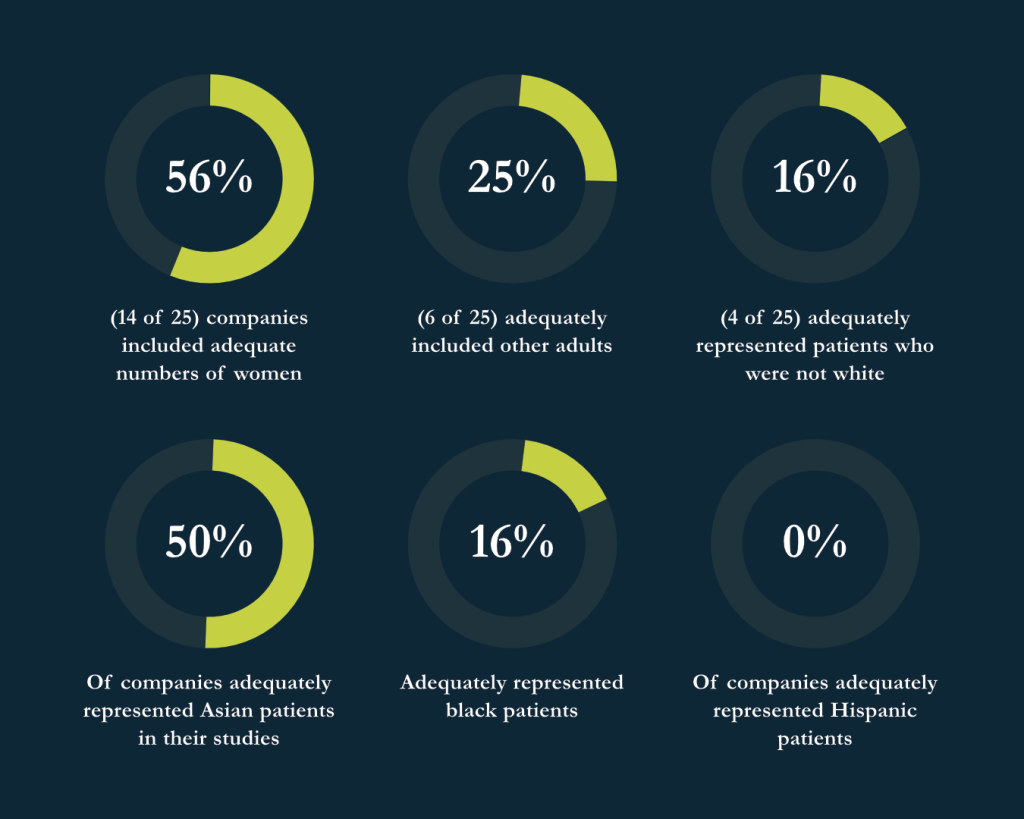
Their research found:
- 56% (14 of 25) companies included adequate numbers of women
- 25% (6 of 25) adequately included older adults
- Just 16% (4 of 25) adequately represented patients who were not white
- Almost 50% of companies adequately represented Asian patients in their studies
- Only 16% adequately represented Black patients
- 0% of companies adequately represented Hispanic patients
The authors of the report stated that they hope their new metric of “fair inclusion,” which combines both inclusion and transparency, will push companies lagging behind to do better. The median company overall fair inclusion score was 81%. Eight companies scored in the top quarter at 87% or above, thereby receiving a gold rating. Five more companies received a silver rating, scoring at or above the median company score.
Specifically, on fair inclusion of women, the median company score was 100% and 14 companies (56%) scored 100%. For overall fair inclusion of older adults, the median company score was 75%, with five companies scoring 100%. For fair inclusion of racially and ethnically minoritised patients, the median company score was 68% and only one company scored 100%.
The study did identify that it had limitations due to some public data on US patient demographics being unavailable and therefore focusing on the use of demographics from the broader cancer types.
Cancer diagnosis trends within the UK and USA pre-2019
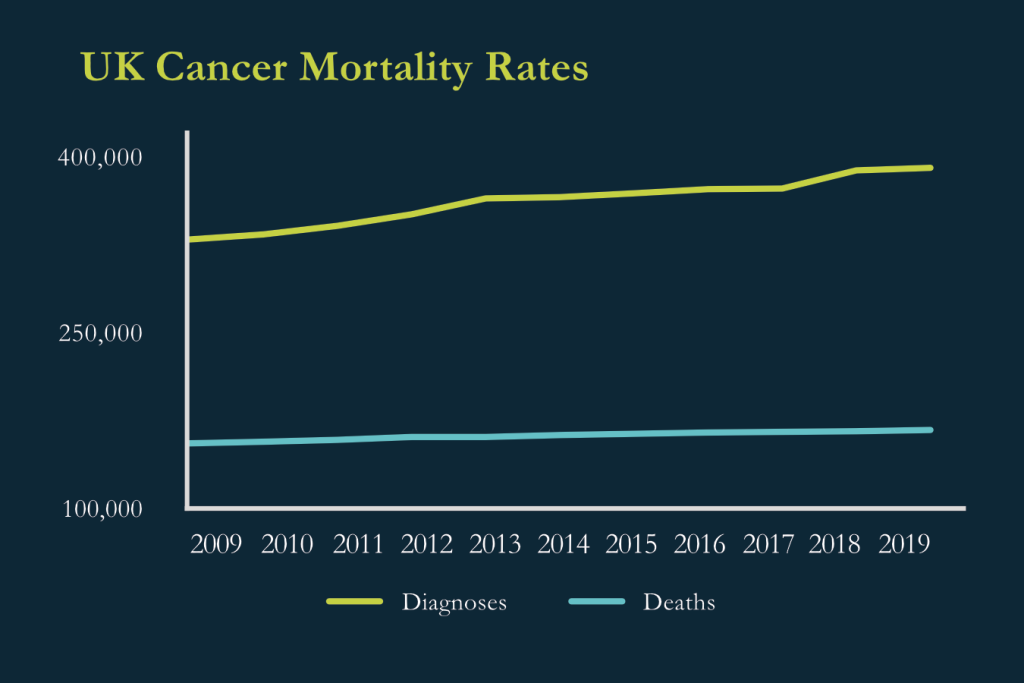
In 2019, around 391,000 people were diagnosed with cancer, in the UK. On average someone is diagnosed with cancer every 90 seconds in the UK. Cancer incidence in the UK has risen by 39% since 2002, and by 19% only in the last decade. This is likely due to the growing and aging population who are at higher risk of developing cancer, as well as improvements in diagnosis initiatives and public awareness. Around 167,000 people died from cancer in the UK in 2019, an average of 460 people every day. However, in comparison to incidence, the number of deaths from cancer in the UK has reported a less dramatic increase, rising by 7% over the previous 10 years. (Macmillan 2022)
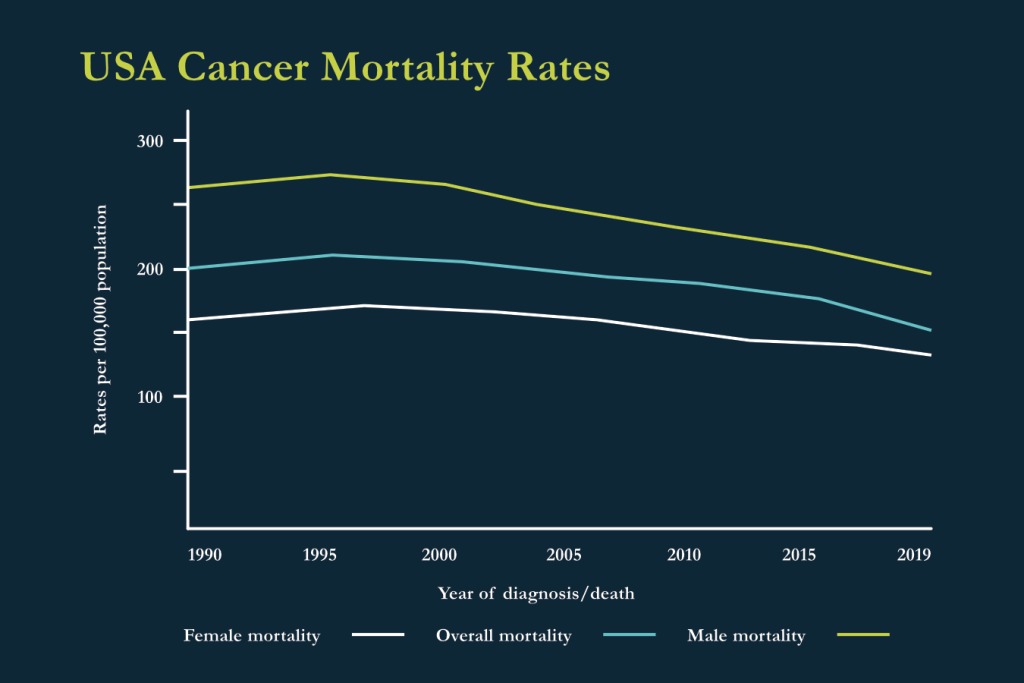
Meanwhile, the USA has seen a 32% drop in the cancer death rate between 1991 and 2019, translating to almost 3.5 million fewer cancer deaths during these years than what would have been expected if the death rate had not fallen. The American Cancer Society suggests that this trend is due to advancements in treatment and early detection.
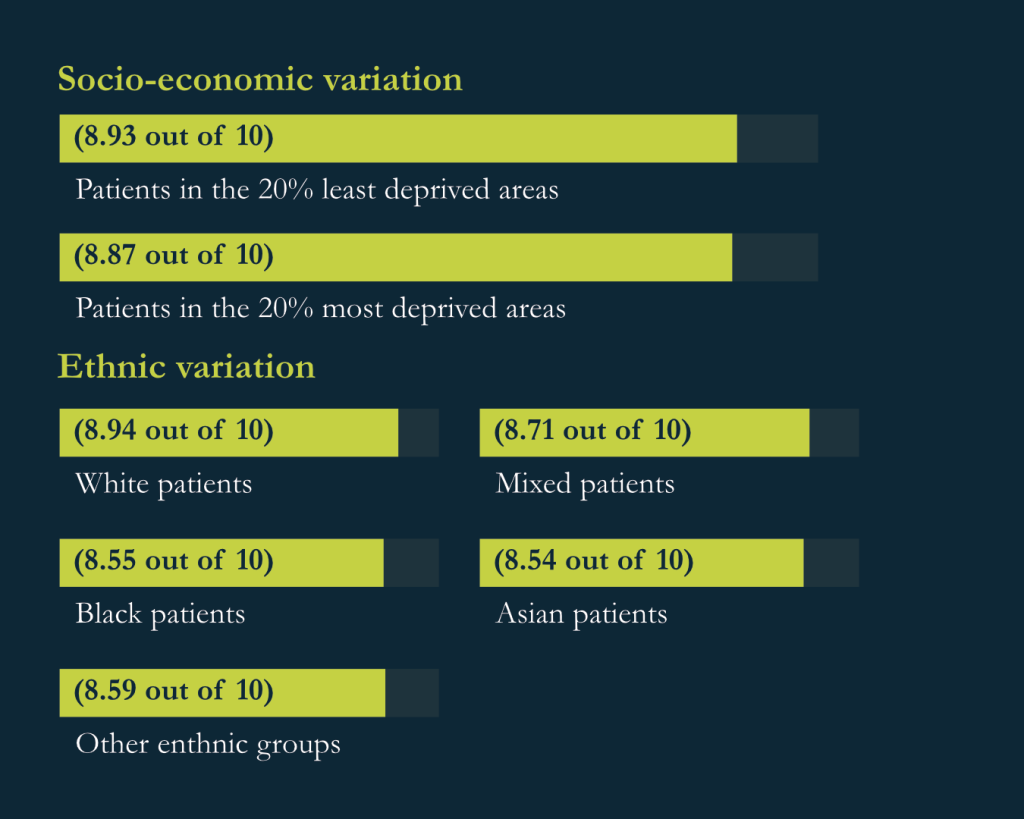
Unfortunately, in terms of variation in experience, analyses of CPES England highlighted the following:
- For socio-economic variation, people from socio-economically deprived areas in England report a worse experience of their cancer care than people from the least deprived areas, with patients in the 20% least deprived areas reporting the highest score for overall care (8.93 out of 10), against patients in the 20% most deprived areas the lowest score (8.87 out of 10).
- In terms of ethnic variation, CPES responses in England have consistently shown, since their first publication in 2010, that people from minority ethnic groups overall report a poorer experience of cancer services than White British people. In 2021, White patients gave a score of 8.94 out of 10 for overall experience of care, in comparison with scores of 8.71 (Mixed), 8.55 (Black), 8.54 (Asian) and 8.59 (Other ethnic groups), within the survey. (Macmillian 2022)
The impact of Covid-19
It is worth bearing in mind that these statistics do not cover the years since the COVID-19 pandemic and the impact it has had within the life sciences industry and healthcare services around the World. While it has posed many challenges, the pandemic has created opportunities to reimagine the way things are done.
While the temporary closures of labs and in-person restrictions slowed research, they also accelerated the development of virtual collaborations, remote testing and treatment approaches. Across the board on a global scale, we have seen how the cancer research community can adapt quickly and that a different future is possible.
The future of clinical cancer trials
In 2021, three key themes emerged at the UK’s largest annual cancer conference, hosted by the NCRI, on the future of clinical cancer trials. These included the following:
- An aging population – Changing demographics mean that by 2035, the world’s population will be much older, delegates at the conference heard. Since cancer incidence increases with age, it is likely that we will see an increase in the number of cancer patients, who will be much older and could have other health problems alongside cancer.
- Radiotherapy – Radiotherapy, for example, is often used in older patients – and, in fact, radiotherapy techniques have advanced hugely and could help tackle some of the challenges posed by an ageing population. Older patients can struggle with side effects though, so anything we can do to minimise those is valuable.
- Drug treatments – Targeted treatments, immunotherapies and drug combinations will be other new options for elderly patients in the future.
Advancements in radiation treatments
Whilst radiation is not a new form cancer treatment, having been used since the early 20th century, despite its benefits it also had its limitations. Too much exposure to radiation could in fact cause cancer therefore outweighing the benefits of being a form of treatment for it. However, advances in radiation physics and computer technology, during the last quarter of the 20th century, has made it possible to aim radiation more precisely.
By focusing radiotherapy in a much more concentrated process, the treatment results have been much more promising.
The increased use of immunotherapy
Traditional immunotherapy has been around for over a century, and the use of it has been to approach cancer by harnessing bacterial or viral infection to enhance immune responses. The connection between tumours and inflammation, was first discovered in 1863, with the earliest case of cancer immunotherapy having been recorded in 1891, when the first attempt to leverage the immune system to treat cancer after noticing that mixtures of live and inactivated Streptococcus pyogenes and Serratia marcescens could cause tumor regression in sarcoma patients.
Although such a pioneering strategy provided a proof of concept for treating cancer by the utilisation of the immune system, the unknown mechanisms of action and the potential infection risks hindered its further progress. Decades later, oncolytic virus therapies were invented, which leverage genetically modified viruses to infect tumour cells, and thus stimulate a proinflammatory environment to augment systemic antitumor immunity.
With advances in genetic engineering and virus transformation technologies, oncolytic virus therapies have made much progress in recent years. In particular, talimogene laherparepvec (T-Vec), also known as Imlygic, a genetically modified herpes simplex virus, demonstrates impressive clinical benefits for patients with advanced melanoma and has been approved for the treatment of unresectable metastatic melanoma.
Cancer vaccines
The success of other immunotherapies has drawn focus away from cancer vaccines, despite their distinct benefits. Although CAR T cells can be effective for cancers with identifiable tumor-specific surface antigens, vaccines have the potential to additionally target the broader set of intracellular antigens. Whereas checkpoint blockade can treat subsets of ‘inflamed’ cancers, infiltrated by previously primed tumor-reactive T cells, cancer vaccines have the potential to newly prime tumor-reactive T cells. Concurrent progress in easier-to-use therapies has also diminished vaccine enthusiasm.
Although five decades of research have yielded many failures, vaccines are now positioned for success for several reasons. Compared to prior decades, it is now clear that (1) T cells can treat (and, in some instances, cure) patients with cancer, as seen with CAR T cells and bispecific T cell engagers; 2) patients’ endogenous T cells can be primed against their own TAAs, correlating with tumor regression, as seen with checkpoint blockade; and 3) priming of endogenous T cells requires optimal antigen presentation (for example, cDC1 cells).
Current insensitive and nonspecific approaches (for example, IFN-γ ELISPOT) are posed to be replaced over the next 5 years with deep immune monitoring approaches to accurately characterize cancer vaccine immune responses. With such means, small trials will be able to quickly identify the most immunologically potent cancer vaccines, thereby avoiding large trials of less immunogenic vaccines. Deep immune monitoring will guide the field on a straightforward trajectory, evaluating the most promising approaches (likely neoantigen and in situ vaccines), to successful, randomized trials and ultimately commercialization. Effective vaccines are likely to be combined with other immunostimulatory approaches including adoptive T cell therapies and to be deployed in postsurgical adjuvant settings to prevent relapses.

Recent updates supporting cancer research
Successful advancements with BIOnTech for the COVID-19 vaccine has seen a number of clinical research trials, currently in progress, examining the potential of adapting it for the use in MRnA cancer vaccines.
The UK Government recently announced that 29 experimental cancer medicine centres (ECMCs) in the UK are to receive £43m in additional support over the next five years to trial new treatments for children and adults. Similar funding has also recently been announced in the USA, with the Weill Cornell Medicine researchers having received a five-year $5.7 million grant, from the National Cancer Institute at the National Institutes of Health, to fund a centre aimed at developing messenger RNA (mRNA) vaccines to deter cancer development in at-risk groups.
Conclusion
Whilst we are seeing promising results from recent clinical trials, we still have a long way to go with seeing this convert into a regular treatment option for cancers. With an aging and expanding population, cancer diagnoses are predicted to increase and therefore research and funding is vital to ensure that we see survival rates continue on an upwards trend. Whilst the impact of the pandemic provided major breakthroughs in research, it is not currently clear overall what the impact it has had on cancer survival rates and may result in a decline in survival rates.
Further research also takes time and therefore we will not see an immediate impact, but it is worth keeping a close eye on how this area develops further. Advancements in research and technology can enhance significant breakthroughs and see developments happen much quicker than anticipated. Another aspect of clinical trial breakthroughs is that diversity and fair representation is considered throughout to ensure that they have the most success.
Sources
- Andrews, M., Bakker, J., Bawagan, J., Bordajandi, D., (2021), The year 2035: What is the future of cancer research and treatment?, The Institute of Cancer Research, URL: https://www.icr.ac.uk/blogs/science-talk/page-details/the-year-2035-what-is-the-future-of-cancer-research-and-treatment
- Baskar R, Yap SP, Chua KL, Itahana K., (2012), The diverse and complex roles of radiation on cancer treatment: therapeutic target and genome maintenance. Am J Cancer Res. URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3410581/
- John Hopkins in Health, (2022), Immunotherapy: Precision Medicine in Action, URL: https://www.hopkinsmedicine.org/inhealth/about-us/immunotherapy-precision-medicine-action-policy-brief.html
- Lin, M.J., Svensson-Arvelund, J., Lubitz, G.S. et al. (2021), Cancer vaccines: the next immunotherapy frontier, Nature.com, URL: https://doi.org/10.1038/s43018-022-00418-6
- Lipkin, S., (2022), CAP-IT Center for LNP RNA Immunoprevention, Weill Cornell Medicene, URL: https://reporter.nih.gov/search/UCo8lWAeaU6jsHha15aNVw/project-details/10505675
- Macmillian Cancer Support. (2022), Statistics and Fact Sheets, URL: Cancer McMillian Stats & Fact Sheet
- McDowell, S., Rausch, S., Simmons, K., (2019), Cancer Research Insights from the Latest Decade, 2010 to 2020, URL: https://www.cancer.org/latest-news/cancer-research-insights-from-the-latest-decade-2010-to-2020.html
- Sample, I., (2023), Cancer centre funding boost to widen UK trials of ‘treatments of the future, The Guardian, URL:https://www.theguardian.com/society/2023/jan/16/cancer-centre-funding-boost-to-widen-uk-trials-of-treatments-of-the-future#:~:text=Doctors%20and%20scientists%20at%2029,prevent%20cancer%20cells%20from%20growing.
- The American Cancer Society, (2014), History of Cancer Treatments: Radiation Therapy. URL: https://www.cancer.org/treatment/understanding-your-diagnosis/history-of-cancer/cancer-treatment-radiation.html
- The American Cancer Society, (2022), Risk of Dying from Cancer Continues to Drop at an Accelerated Pace, URL: https://www.cancer.org/latest-news/facts-and-figures-2022.html
- University of Oxford (2021), Vaccine for treating cancer made possible using Oxford COVID vaccine technology, URL: https://www.ox.ac.uk/news/2021-09-03-vaccine-treating-cancer-made-possible-using-oxford-covid-vaccine-technology
- Varma T., Mello M., Ross J.S., et. al., (2023), Metrics, baseline scores, and a tool to improve sponsor performance on clinical trial diversity: retrospective cross sectional study, BMJ Medicine, URL: https://bmjmedicine.bmj.com/content/2/1/e000395.info
- Walsh, F., (2022), BioNTech: Could Covid vaccine technology crack cancer?, BBC, URL: https://www.bbc.co.uk/news/health-63247997
- Weill Cornell Medicene, (2022), NIH Grant Funds Cancer Prevention Vaccine Research, Weill Cornell Medicene, URL: https://news.weill.cornell.edu/news/2022/11/nih-grant-funds-cancer-prevention-vaccine-research
- World Cancer Day, (2022), Campaign Theme: Close the Care Gap, World Cancer Day, URL: https://www.worldcancerday.org/about/2022-2024-world-cancer-day-campaign
- Zhang, Y., Zhang, Z., (2020), The history and advances in cancer immunotherapy: understanding the characteristics of tumor-infiltrating immune cells and their therapeutic implications, Nature.com, URL: https://www.nature.com/articles/s41423-020-0488-6#:~:text=The%20earliest%20case%20of%20cancer,cause%20tumor%20regression%20in%20sarcoma